手术jones骨折第5跖骨基底骨折切开复位内固定术.docx
《手术jones骨折第5跖骨基底骨折切开复位内固定术.docx》由会员分享,可在线阅读,更多相关《手术jones骨折第5跖骨基底骨折切开复位内固定术.docx(12页珍藏版)》请在冰豆网上搜索。
手术jones骨折第5跖骨基底骨折切开复位内固定术
Jonesmann骨折指第五跖干骺端与骨干连接部骨折。
英国骨科医生Sir Robert Jones(1857–1933)自己跳舞后发生此类骨折并首先描述,故此得名。
Jonesfracturesoccurinasmallareaofthefifthmetatarsalthat receiveslessblood andisthereforemorepronetodifficultiesinhealing.AJonesfracturecanbeeitherastressfracture(atinyhairlinebreakthatoccursovertime)oranacute(sudden)break.Jonesfracturesarecausedbyoveruse,repetitivestress,ortrauma.Theyarelesscommonandmoredifficulttotreatthanavulsionfractures.
A Jonesfracture isa fracture ofthe diaphysis ofthe fifthmetatarsal ofthe foot.Thefifthmetatarsalisatthebaseofthesmall toe.The proximalend,wheretheJonesfractureoccurs,isinthemidportionofthefoot.PatientswhosustainaJonesfracturehave pain overthisarea,swelling,anddifficultywalking.Thefracturewasfirstdescribedby British orthopedicsurgeonSir RobertJones,whosustainedthisinjuryhimselfwhiledancing,inthe AnnalsofSurgery in1902.
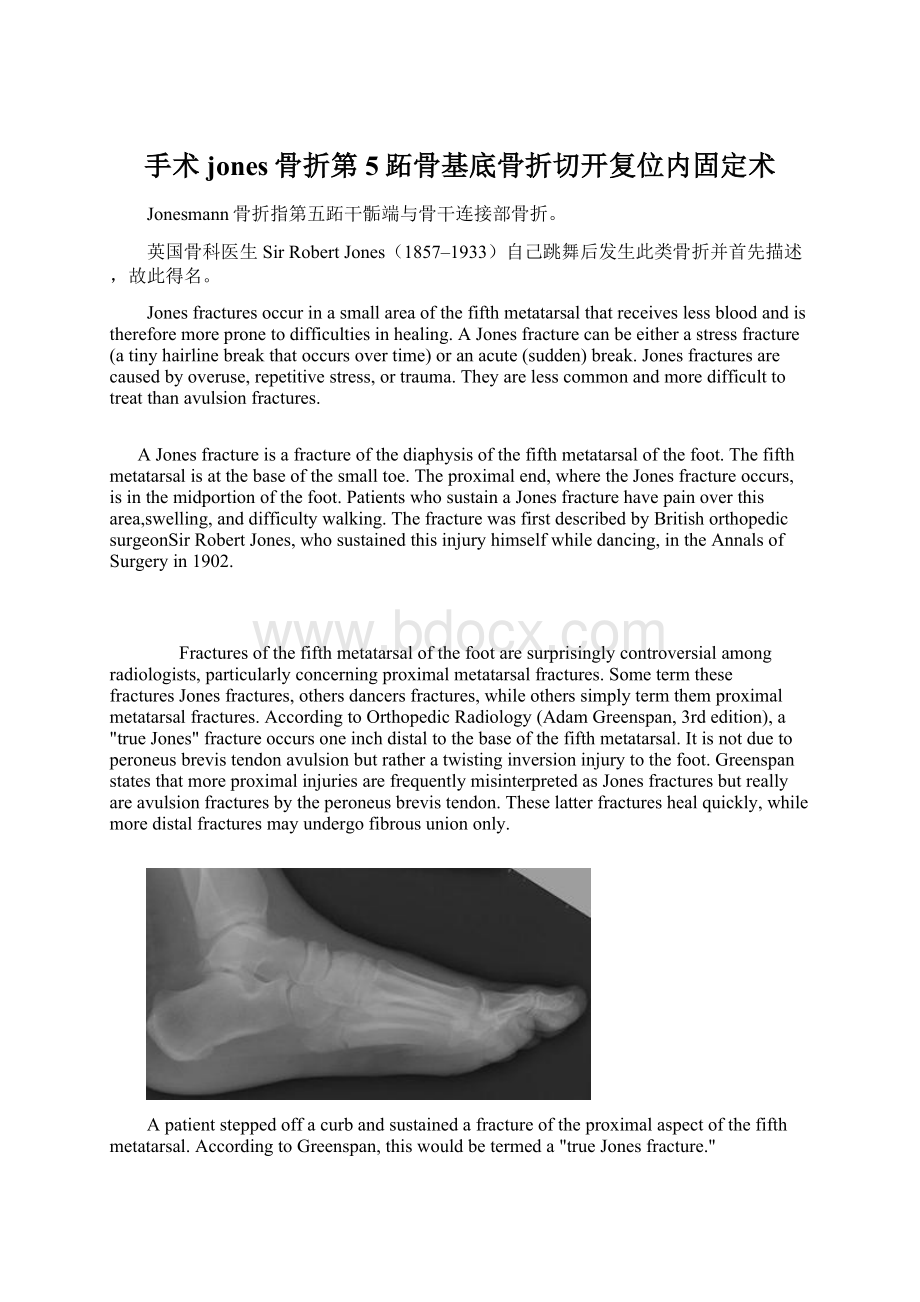
Fracturesofthefifthmetatarsalofthefootaresurprisinglycontroversialamongradiologists,particularlyconcerningproximalmetatarsalfractures.Sometermthesefractures Jonesfractures,others dancersfractures,whileotherssimplytermthem proximalmetatarsalfractures.AccordingtoOrthopedicRadiology(AdamGreenspan,3rdedition),a"trueJones"fractureoccursoneinchdistaltothebaseofthefifthmetatarsal.Itis notduetoperoneusbrevistendonavulsionbutratheratwistinginversioninjurytothefoot.GreenspanstatesthatmoreproximalinjuriesarefrequentlymisinterpretedasJonesfracturesbutreallyareavulsionfracturesbytheperoneusbrevistendon.Theselatterfractureshealquickly,whilemoredistalfracturesmayundergofibrousuniononly.
Apatientsteppedoffacurbandsustainedafractureoftheproximalaspectofthefifthmetatarsal.AccordingtoGreenspan,thiswouldbetermeda"trueJonesfracture."
Incontradistinction,thispatientsustainedafractureoftheproximalaspectofthefifthmetatarsal.Greenspantermsthisanavulsioninjury.Inanavulsionfracture,asmallpieceofboneispulledoffthemainportionofthebonebyatendonorligament.Thistypeoffractureistheresultofaninjuryinwhichtheanklerolls.Avulsionfracturesareoftenoverlookedwhentheyoccurwithananklesprain.
Treatment:
IfaJonesfractureisnotsignificantlydisplaced,itcanbetreatedwitha cast,splintorwalkingbootforfourtoeightweeks.Patientsshouldnotplaceweightonthefootuntilinstructedbytheirdoctor.Three-fourthsoffracturestreatedlikethisshouldheal.
Inthecaseofacutefractureinanathlete,adynamiccompressionplatecanbeplacedonthetensionsideofthefracture,K-WirewithMonofiamentwireinafigure8fashionduetothenatureofatransversefracture.Internalfixationwithcorticalorcancellousscrewwouldrequireanobliquefracturethatcouldbeaddressedthrough"Theruleof2's"inregardstoInternalfixationwithscrews.
Othertreatmentscommonlyencouragedareincreasedintakeof vitaminD and calcium.
Thisinjurymustbedifferentiatedfromthephysiologicdevelopmental apophysis commonlyandnormallyoccurringatthissiteinadolescents.Differentiationispossiblebycharacteristicssuchasabsenceofsclerosisofthefracturededges(inacutecases)andorientationofthelucentline:
transverse(at90degrees)tothemetatarsalaxisforthefracture(duetoavulsionpullbytheperoneusbrevismuscleinsertingattheproximaltip)-andparalleltothemetatarsalaxisinthecaseoftheapophysis.
Jonesfracturescanbecomechronicconditionsifthefracturefailstounite,orheal.Ifthisisthecase,surgerywilllikelyberecommendedtosecurethefractureinplacewithascrew,andbonegraftmaybeusedtostimuateahealingresponse.
-SurgicalTreatment:
(JonesFrx);
-patientispositioninpartiallateralpositiononbeanbag;
- flouroscopy:
-underflourscopicguidence,aKwireisinsertedfordeterminationofproperpositionandlength;
- mostcommonmistakeistodirectthedrillplantarly,ratherthanparallelw/theshaftofmetatarsal;
- secondmistakeistoopositiontheguidewireusingtheobliqueview;
-notethatthemetatarsalshaftismorenarrowontheAPview,anditis possibleforthepintobecenteredontheobliqueview
whereasonAPviewthepiniseccentricallypositioned;
- incision:
-longitudinalincisionismadeoverdistalmetatarsal;
-takecaretoavoidbranchesofthesuralnervewhichcancoursedorsally,andlaterallyovermetatarsal;
-peroneusbrevisisretractedinferiorly;
- insertionofthistendonmayobscuretheproperdrillentrysite;
- localbonegraft:
-canbeobtainedfromtuberosityandfrombonebitsfromthedrill;
- implants:
-considerinsertionof 4.5cancellousbonescrews, 4.5mmcannulatedscrews(whichareusedinmostcases)buthave available5.5cannulated(and solid) screwsand6.5mmcannulatedscrews;
-diametershoulddependonwidthofthecanal(letthescrewtaphelpdeterminethebestsize);
-ineithercase,threadsmustcrossthefrxline;
-lengthisusuallybetween40-55mm;
-considercountersinkingthescrewtoavoidprominenceofthescrewhead;
-in reportbyIPKelly, authorsnotedthatfailureismorelikelywhensmallerdiameterscrews areused;
-experimentalJonesfractureswerecreatedin23pairsofhumancadaverfifthmetatarsals,whichwerefixedusingeither5.0mmor6.5mmscrews;
-frxstiffnessandpull-outstrengthsweremeasuredforeitherscrewtypeand relationshipswithbone densityand canaldiameterweredetermined;
-poorthreadpurchasewithinthemedullarycanalwasnotedwiththe5.0mmscrews,whileexcellentpurchasewasnotedwith6.5mmscrews;
-pull-outstrengthtestingrevealedsignificantlyhigherpulloutstrengthsforthelarger6.5mmscrews;
-theauthorsconcludethatlargerdiameterscrewsmaybemoreappropriateforintramedullaryscrewfixationofJonesfractures;
-ref:
TreatmentofJonesFractureNonunionsandRefracturesintheEliteAthleteOutcomesofIMScrewFixationWithBoneGrafting
- postop:
patientswill requireprotectedpostoperative wtbearing;
1、解剖方面考虑:
恢复跖骨头的队列关系是非常重要的前足的力学目标:
如下图示:
在正位,应是“顺流而下”的表现,且与对侧足对称,这是恢复正常跖骨长度的保证。
另一个需要恢复的重要结构是跖骨水平线,需保持其均在一个水平线上。
需要注意的是,在第一跖骨,是籽骨在承重,而不是第一跖骨头,因此,序列对应关系应与籽骨为准。
任何力线改变均可引起站立相和推离相时疼痛及胼胝形成。
2、螺钉或钢板固定:
固定这种骨折,因尽可能使其稳定。
横行骨折线时,单独拉力螺钉固定即可。
3、手术入路:
详见后。
4、复位:
骨折在直视下复位,因为其为横形骨折,复位满意后用复位钳保持复位。
5、拧入螺钉:
从腓骨短肌肌腱止点处,稍向内侧倾斜方向打入导针,这样可以抓住远骨折端的内侧骨皮质,增加稳定。
骨折近端应做成滑动孔,以允许骨折块间加压,螺钉直径应根据骨情况来选择,常选用3.5或4.0mm螺钉固定。
6、另一种固定方式:
髓内螺钉固定:
选髓内螺钉固定,螺钉直径要与髓腔匹配,螺钉必须有充足直径以获得稳定加压固定,根据髓腔的大小,可选用3.5或4.5mm皮质螺钉固定,在体型高大患者,可能需用6.5mm松质骨螺钉固定。
1、注意保护血运:
避免广泛深度暴露、过度牵拉;多个跖骨骨折应采用单独切口,避免增加软组织损伤;在足部保护静脉回流是非常重要的。
2、解剖:
小隐静脉位于切口部位的皮下;在静脉的深面是小趾外展肌;腓肠神经(与小隐静脉伴行)的分支应给予保护。
3、皮肤切口:
切口开始于可触及的第5跖骨茎突处,依据需要向远端延伸。
切口要位于足部掌侧皮肤与背侧皮肤的交界处。
4、深层分离:
显露第5小趾外展肌筋膜,并纵向切开。
5、骨质显露:
使用拉钩,向背侧牵开皮肤及背侧筋膜,向掌侧牵开肌肉,显露第5跖骨基底。
 升级会员
升级会员 