Review article.docx
《Review article.docx》由会员分享,可在线阅读,更多相关《Review article.docx(41页珍藏版)》请在冰豆网上搜索。
Reviewarticle
Reviewarticle
Diagnosisandtreatmentofasthmainchildhood:
aPRACTALLconsensusreport
Asthmaistheleadingchronicdiseaseamongchildreninmostindustrializedcountries.However,theevidencebaseonspecificaspectsofpediatricasthma,includingtherapeuticstrategies,islimitedandnorecentinternationalguidelineshavefocusedexclusivelyonpediatricasthma.Asaresult,theEuropeanAcademyofAllergyandClinicalImmunologyandtheAmericanAcademyofAllergy,AsthmaandImmunologynominatedexpertteamstofindaconsensustoserveasaguidelineforclinicalpracticeinEuropeaswellasinNorthAmerica.Thisconsensusreportrecommendsstrategiesthatincludepharmacologicaltreatment,allergenandtriggeravoidanceandasthmaeducation.ThereportispartofthePRACTALLinitiative**,whichisendorsedbybothacademies.
评论文章
童年哮喘的诊断和治疗:
一个PRACTALL共识报告
在大多数工业国家,哮喘是首要的儿童慢性病,然而,建立在儿童哮喘特殊方面的证据,包括治疗措施,是有限的,而且没有最近的国际方针仅仅重点在儿童哮喘。
结果,欧洲过敏和免疫学院和美国过敏,哮喘和免疫学院提名专家组来找到一个共识作为欧洲和北美的一个临床实践指引。
这个共识报告推荐策略包括药理治疗,过敏原和避免触发以及哮喘教育。
这个报告是PRACTALL的一部分,得到两个学院的赞同。
Abbreviations:
ACT,AsthmaControlTest;DPI,drypowderinhaler;eNO,exhalednitricoxide;FEF,forcedexpiratoryflow;FEV1,forcedexpiratoryvolume;FVC,forcedvitalcapacity;GP,generalpractitioners;HPA,hypothalamic–pituitary–adrenal;ICS,inhaledcorticosteroids;IgE,immunoglobulinE;IL,interleukin;LABA,long-actingb2receptoragonist;LTRA,leukotrienereceptorantagonist;MDI,metereddoseinhaler;nNO,nasalnitricoxide;PEF,peakexpiratoryflow;SLIT,sublingualimmunotherapy
Bacharieretal.
缩写:
ACT哮喘控制试验,DPI干粉吸入器,eNO呼出的一氧化碳,FEF,用力呼气流量,FEV1用力呼气容积,FVC用力肺活量,GP普通科医生,HPA下丘脑-垂体-肾上腺,ICS吸入皮质类固醇,IgE免疫球蛋白E,IL白细胞介素,LABA长效β2受体激动剂,LTRA白三烯受体拮抗剂,MDI计量吸入器,
nNO鼻一氧化氮,PEF呼气流速峰值,SLIT舌下含服免疫疗法
Bacharier等人
Asthmaisthemostcommonchronicchildhooddiseaseinnearlyallindustrializedcountries.Itismoreprevalentinchildrenwithafamilyhistoryofatopy,andsymptomsandexacerbationsarefrequentlyprovokedbyawiderangeoftriggersincludingviralinfections,indoorandoutdoorallergens,exercise,tobaccosmokeandpoorairquality.Manyinfantsandpreschoolchildrenexperiencerecurrentepisodesofbronchialsymptoms,especiallywheezingandcough,beginningatafewmonthsofage,mainlyduringalowerrespiratorytractinfection,andsinceaclinicaldiagnosisofasthmausuallycanbemadewithcertaintybyage5,theearlydiagnosis,monitoringandtreatmentofrespiratorysymptomsareessential.
哮喘在几乎所有的工业国家中是最常见的儿童时期慢性病。
它盛行在有家族过敏体质的儿童中,而且症状和病情加重经常因广泛的触发器激动包括,室内和室外过敏原,运动,吸入尼古丁和差的空气质量。
许多婴儿和学龄前儿童经历支气管症状的反复发作,特别是喘息和咳嗽,开始于几个月的年龄,主要是在一个下呼吸道感染的过程中,而且自从哮喘通常是自5岁后才被诊断,早期的诊断,监测和治疗呼吸道症状是必要的。
Atthetimeofthisreport,therearefewnational(1–4)andnoup-to-dateinternationalguidelines(5)thatfocusexclusivelyonpediatricasthma,eventhoughchildrenhaveahigheroverallprevalenceofasthmacomparedtoadults.Pharmacotherapyforchildhoodasthmahasbeendescribedingeneralasthmaguidelines,includingtherecentlyupdatedGlobalInitiativeforAsthma(GINA)guidelines(6)andinsomenationalguidelines.However,theinformationavailableonspecificaspectsofpediatricasthma,inparticularinchildrenunder5yearsofage,islimitedanddoesnotincludetheopinionandcontributionsofthepediatricallergyandrespiratorycommunity(1,7,8).Incontrasttoadults,theevidencebaseforpharmacotherapyinchildrenunder5yearsofageisverysparse.ThecurrentBritishThoracicSocietyGuideline(9)hasbeenthemostaccessiblesourceofinformationfortreatmentofpediatricasthma,withrecommendationsbasedontheavailableliteratureandwhereevidenceislackingonexpertopinion.
在本报告的时间,这里有少许全国性的(1-4)和没有到日期的国际性的方针(5)专注于儿科哮喘,和成人比儿童哮喘更盛行,药物治疗儿童哮喘是在普通哮喘方针中描述,包括最近更新的全球哮喘防治(GINA)方针(6)和在一些全国的方针。
然而,能从儿科哮喘的特殊方面获得的信息,特别是在5岁以下儿童,是有限的而且不包括儿科过敏和呼吸社区的意见和贡献(1,7,8)。
和对比成人,建立在5岁以下儿童药物治疗基础上的证据是很稀少的。
现在英国胸椎社会方针(9)已经是在治疗儿科哮喘中最能够得到的信息资源,伴随着可用的文学推荐和缺少专家意见的证据。
Inviewofthelimiteddatafromrandomizedcontrolledtrialsinchildrenandthedifficultiesinapplyingsystematicreviewcriteriatodiagnosis,prognosisandnonpharmacologicalmanagement,thisreportemployedaconsensusapproachbasedonavailablepublishedliterature(June2007)andonbestcurrentclinicalpractice.Thereportreviewsthenaturalhistoryandpathophysiologyofpediatricasthmaandprovidesrecommendationsfordiagnosis,practicalmanagementandmonitoring.Therecommendationsareaimedatbothpediatriciansandgeneralpractitioners(GPs)workinginhospitals,officeorprimarycaresettings.
鉴于从儿童随机对照试验得到的有限的数据和应用系统的审查标准来诊断,预后和非药物管理的困难,这个报告根据可供公开发表的文献使用了协商一致的办法(到2007年6月为止)在最好的现在临床实践。
报告复习了儿科哮喘的自然史和病理生理学,提供诊断,实践管理和监视的建议。
建议旨在工作在医院的儿科医生和从业人员(GPs),办公室或基层医疗服务的设置。
NaturalhistoryAsthmainchildrencanbedescribedas_repeatedattacksofairwayobstructionandintermittentsymptomsofincreasedairwayresponsivenesstotriggeringfactors,suchasexercise,allergenexposureandviralinfections_(10).However,thedefinitionbecomesmoredifficulttoapplyconfidentlyininfantsandpreschoolagechildrenwhopresentwithrecurrentepisodesofcoughingand/orwheezing.Althoughthesesymptomsarecommoninthepreschoolyears,theyarefrequentlytransient,and60%ofchildrenwithinfantilewheezewillbehealthyatschoolage(11).Physiciansshouldmanageandexcludediagnosesotherthanasthma,andbeawareofthevariablenaturalhistorypatternsofrecurrentwheezinginearlychildhood.Threedifferentpatternsofrecurrentwheezeinpediatricpatientshavebeenproposed(12),andafourthwasrecentlydescribed(13).However,itshouldbenotedthatpatterns1and2(listedbelow)canonlybediscriminatedretrospectivelyandarenotsuitableforusewhentreatingthechild.
儿童哮喘的自然史可以被描述为反复发作的气道阻塞和间歇性气道反应性增加的症状作为触发因子。
比如运动,过敏原暴露和病毒感染(10),然而,在婴儿和学龄前儿童正在经历反复发作的咳嗽和或/喘息。
虽然这些症状在学龄前是很常见的,它们常常是短暂的,而且60%的儿童在婴儿时期出现过喘息在学龄期会变得健康(11)。
医生应该管理和排除哮喘的诊断,做到对儿童早期的反复发作的喘息心中有数。
儿科病人的三个不同的反复发作喘息的模式已经被建议(12),第四个最近被描述(13),然而,注意模式1和2(见下列)只能追溯歧视但不适合用于治疗儿童。
1.Transientwheezing:
Childrenwhowheezeduringthefirst2–3yearsoflife,butdonotwheezeaftertheageof3years
2.Nonatopicwheezing:
Mainlytriggeredbyviralinfectionandtendstoremitlaterinchildhood
3.Persistentasthma:
Wheezingassociatedwiththefollowing:
•Clinicalmanifestationsofatopy(eczema,allergicrhinitisandconjunctivitis,foodallergy),bloodeosinophilia,and/orelevatedtotalimmunoglobulinE(IgE)
•SpecificIgE-mediatedsensitizationtofoodsininfancyandearlychildhood,andsubsequentlytocommoninhaledallergens(14–18)
•Inhalantallergensensitizationpriorto3yearsofage,especiallywithsensitizationandhighlevelsofexposuretospecificperennialallergensinthehome(10)
•Aparentalhistoryofasthma(15)
4.Severeintermittentwheezing(13):
Infrequentacutewheezingepisodesassociatedwiththefollowing:
•Minimalmorbidityoutsideoftimeofrespiratorytractillness
•Atopiccharacteristics,includingeczema,allergicsensitizationandperipheralbloodeosinophilia
1.瞬态喘息:
儿童在初生的2~3年喘息,但是在3岁以后不再喘息。
2.非过敏体质的喘息:
主要由病毒感染触发,在儿童时代的后期趋于缓和
3.持久性哮喘:
喘息与以下有关:
过敏体质的临床表现(湿疹,过敏性鼻炎和结膜炎,食物过敏),血液中嗜酸性粒细胞浸润,和/或升高的总免疫球蛋白E(IgE)
婴儿和早期儿童特异的IgE介导的食物过敏,和随后的对常见的吸入过敏原过敏(14-18)
3岁前吸入性过敏原过敏,特别是过敏和在家中高暴露于特殊长期过敏原(10)
父母有哮喘史(15)
4.严重的间歇性喘息(13):
偶发的与下列相关的急性发作的喘息
呼吸道疾病以外的时间最小的发病率
过敏体质特征,包括湿疹,过敏性致敏和外周血嗜酸性粒细胞浸润
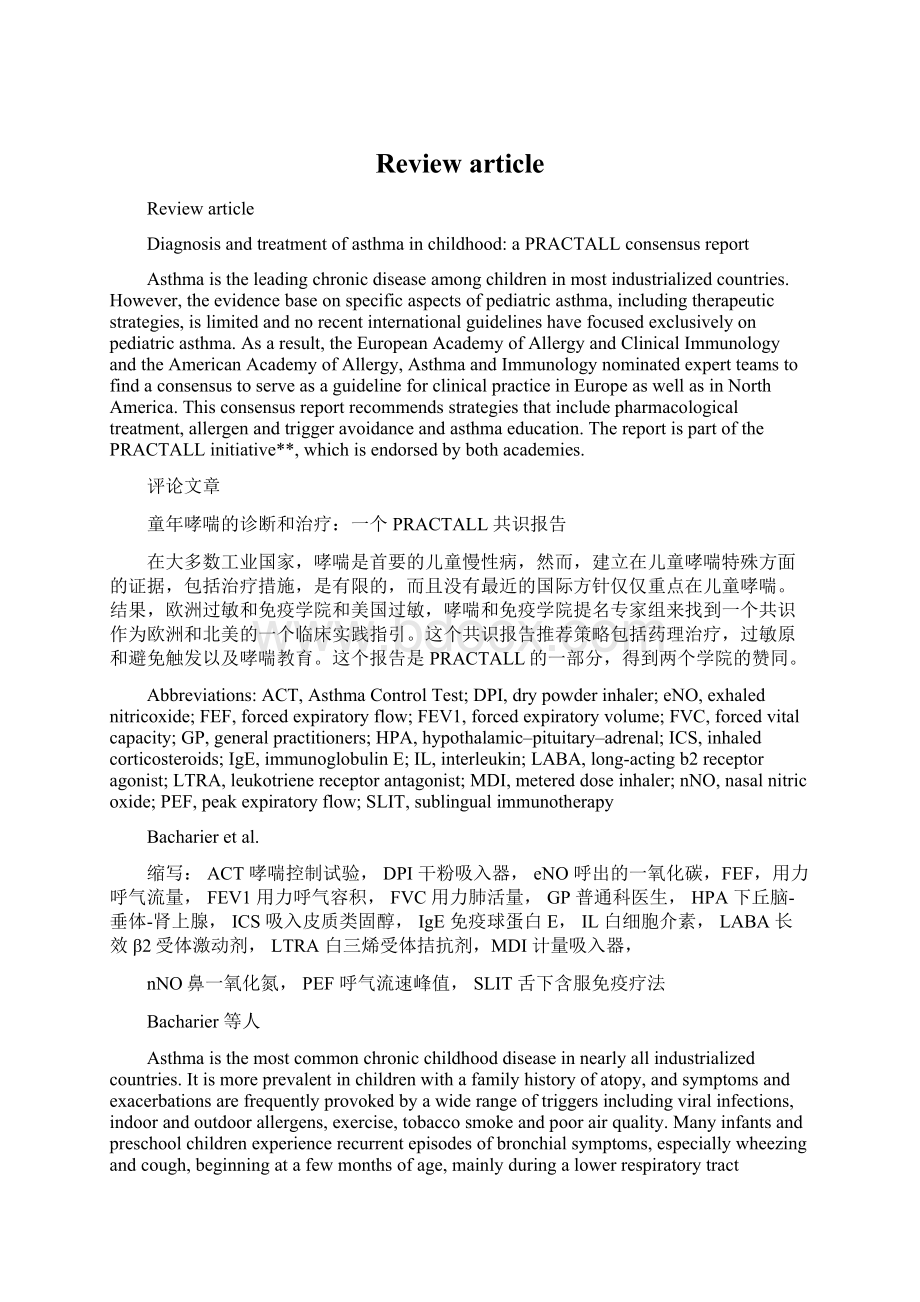
Thehighestincidenceofrecurrentwheezingisfoundinthefirstyearoflife.Accordingtolong-termpopulationrelatedprospectivebirthcohortstudies,upto50%ofallinfantsandchildrenbelowtheageof3yearswillhaveatleastoneepisodeofwheezing(19).Infantswithrecurrentwheezinghaveahigherriskofdevelopingpersistentasthmabythetimetheyreachadolescence,andatopicchildreninparticulararemorelikelytocontinuewheezing(Fig.1)(10).Inaddition,theseverityofasthmasymptomsduringthefirsttwoyearsoflifeisstrongly
relatedtolaterprognosis(20).However,boththeincidenceandperiodprevalenceofwheezingdecreasesignificantlywithincreasingage(12).
经常性喘息的发病率最高是在生命的第一年。
根据长远的人口相关的准出生队列研究,达到50%的所有婴儿和3岁以下的儿童将会有至少一集的喘息(19)。
有反复发作喘息的婴儿在他们到达青春期时有发展持续性喘息的高危险,尤其是过敏体质儿童更有可能继续喘息(Fig.1)(10).此外,生后头两年的哮喘症状严重程度和后来预后非常有关(20).然而,喘息疾病的发病率和持续时间显著与增加的年龄有关(12)
Figure1.Prevalenceofcurrentwheezefrombirthtoage13yearsinchildrenwithanywheezingepisodeatschoolage(5–7years),stratifiedforatopyatschoolage(10).
图1,目前从出生到13岁儿童在任何学龄(5-7岁)喘息情况喘息的患病率,在上学的年龄为过敏体质
Determinants
决定因素
Geneticfactors.Studiesonmono-anddizygotictwinsalongwiththeassociationofasthmaphenotypewithinfirstdegreerelativessuggestageneticbasistoasthma.Morerecently,genomewidescreensfollowedbypositionalcloningandcandidategeneassociationstudieshaveidentifiedgeneticlocirelatedtoincreasedriskofasthmaincertainpopulations(21).Theeffectofgeneticvarianceonasthmaandasthma-relatedphenotypesshowsagreatdealofheterogeneity,andmaybestronglyinfluencedbyenvironmentalfactors(22–24).Accordingly,manychildrenwhodevelopasthmadonothaveparentswithasthma,andmanyparentswithasthmahavechildrenwhodonotdevelopasthma(10).Moststudiesontheincidenceandprevalenceofasthmainchildhoodhaveindicatedthattheprevalenceishigherinboysthaningirlsinthefirstdecadeoflife(25,26),althoughoneserialcross-sectionalstudyhassuggestedarecentnarrowingofthisgendergap(27).However,aschildrenapproachtheteenageyears,new-onsetasthmabecomesmorecommoningirlsthanboys,especiallyinthosewithobesityandearly-onsetpuberty(28).Thereasonforthesegenderdifferencesisnotwellunderstood
基因因素。
研究单和异卵双胞胎随着哮喘表型协会在一级亲属暗示对哮喘有基因基础。
最近,全基因组屏幕跟随着定位克隆和候选基因研究确定基因位点和增加的哮喘危险在特定的人群中(21)。
哮喘的
 升级会员
升级会员 