Appendicitis.docx
《Appendicitis.docx》由会员分享,可在线阅读,更多相关《Appendicitis.docx(13页珍藏版)》请在冰豆网上搜索。
Appendicitis
Appendicitis
FromWikipedia,thefreeencyclopedia
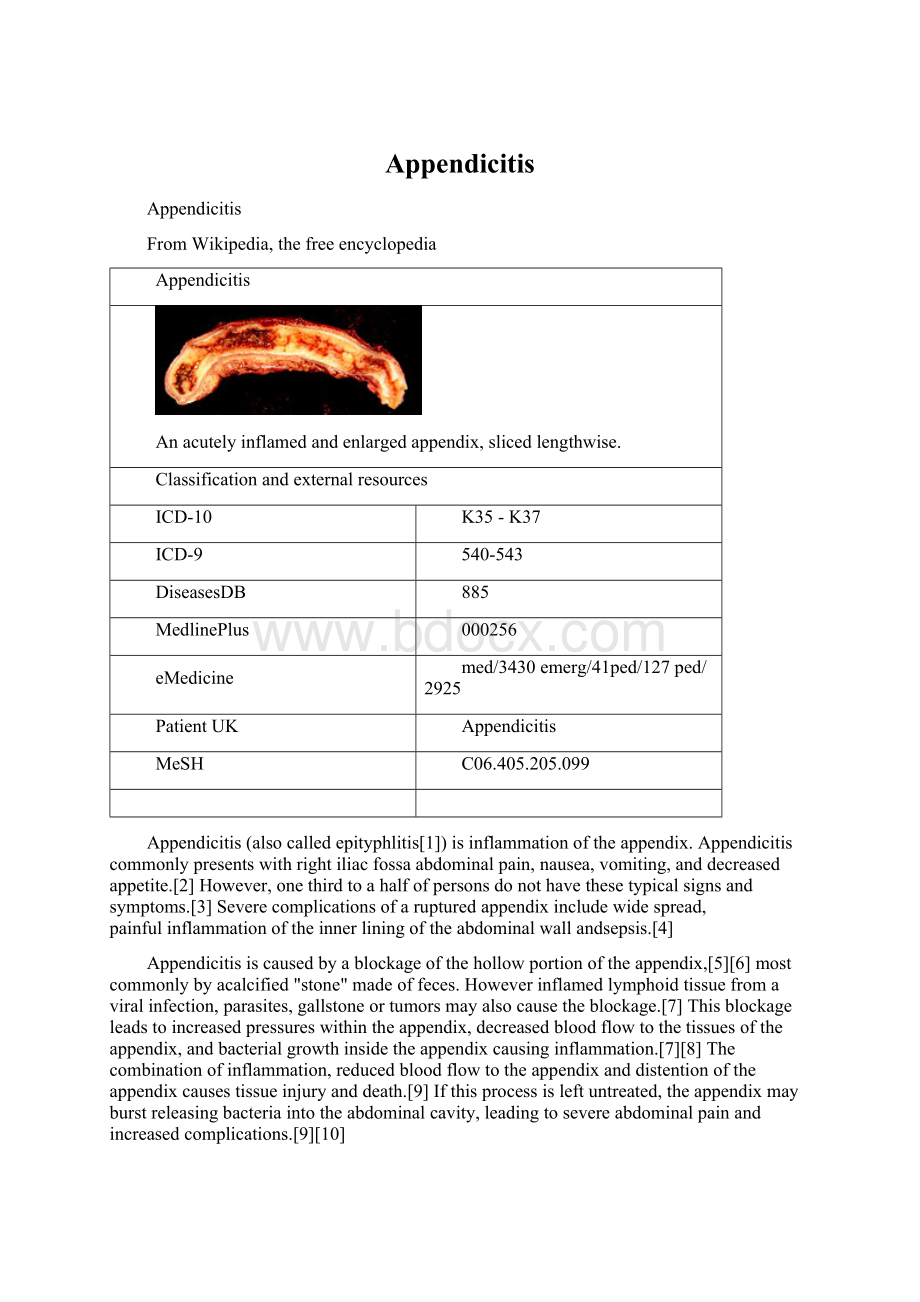
Appendicitis
Anacutelyinflamedandenlargedappendix,slicedlengthwise.
Classificationandexternalresources
ICD-10
K35 - K37
ICD-9
540-543
DiseasesDB
885
MedlinePlus
000256
eMedicine
med/3430 emerg/41ped/127 ped/2925
PatientUK
Appendicitis
MeSH
C06.405.205.099
Appendicitis (alsocalled epityphlitis[1])is inflammation ofthe appendix.Appendicitiscommonlypresentswithright iliacfossa abdominalpain, nausea, vomiting,and decreasedappetite.[2] However,onethirdtoahalfofpersonsdonothavethesetypicalsignsandsymptoms.[3] Severecomplicationsofarupturedappendixincludewidespread,painful inflammationoftheinnerliningoftheabdominalwall andsepsis.[4]
Appendicitisiscausedbyablockageofthe hollowportion oftheappendix,[5][6] mostcommonlybyacalcified"stone"madeoffeces.Howeverinflamed lymphoidtissue fromaviralinfection, parasites,gallstoneor tumors mayalsocausetheblockage.[7] Thisblockageleadstoincreasedpressureswithintheappendix,decreasedbloodflowtothetissuesoftheappendix,andbacterialgrowthinsidetheappendixcausinginflammation.[7][8] Thecombinationofinflammation,reducedbloodflowtotheappendixanddistentionoftheappendixcausestissueinjuryanddeath.[9] Ifthisprocessisleftuntreated,theappendixmayburstreleasingbacteriaintotheabdominalcavity,leadingtosevereabdominalpainandincreasedcomplications.[9][10]
Thediagnosisofappendicitisislargelybasedontheperson'ssignsandsymptoms.[8] Incaseswherethediagnosiscannotbemadebasedontheperson'shistoryandphysicalexam,closeobservation,radiographicimagingandlaboratorytestscanoftenbehelpful.[11] Thetwomostcommonimagingtestsusedare ultrasoundand computertomography (CTscan).[11] CTscanhasbeenshowntobemoreaccuratethanultrasoundindetectingacuteappendicitis.[12][13] However,ultrasoundmaybepreferredasthefirstimagingtestinchildrenandpregnantwomenduetotherisksassociatedwithradiationexposurefromCTscans.[11]
Thestandardtreatmentforacuteappendicitisis surgicalremovaloftheappendix.[7][8] Thismaybedonebyan openincisionintheabdomen orthroughafew smallerincisionswiththehelpofcameras.Surgerydecreasestheriskofsideeffectsordeathassociatedwithruptureoftheappendix.[4] Antibiotics maybeequallyeffectiveincertaincasesofnon-rupturedappendicitis.[14] Itisoneofthemostcommonandsignificantcausesofsevereabdominal pain thatcomesonquickly worldwide.In2013itresultedin72,000deathsglobally.[15] IntheUnitedStates,appendicitisisthemostcommoncauseofacuteabdominalpainrequiringsurgery.[2] EachyearintheUnitedStates,morethan300,000personswithappendicitishavetheirappendixsurgicallyremoved.[16] ReginaldFitz iscreditedwithbeingthefirstpersontodescribetheconditioninapaperpublishedin1886.[17]
Contents
[hide]
∙1 Signsandsymptoms
∙2 Causes
∙3 Diagnosis
o3.1 Clinical
o3.2 Bloodandurinetest
o3.3 Imaging
o3.4 Scoringsystems
o3.5 Pathology
o3.6 Differentialdiagnosis
∙4 Management
o4.1 Pain
o4.2 Surgery
∙5 Prognosis
∙6 Epidemiology
∙7 Societyandculture
o7.1 Lengthofstay
∙8 References
∙9 Externallinks
Signsandsymptoms[edit]
Locationoftheappendixinthedigestivesystem
Painfirst,nauseaandvomitingnext,andfeverlasthasbeendescribedastheclassicpresentationofacuteappendicitis.Becausetheinnervationoftheappendixentersthe spinalcord atthesamelevelasthe umbilicus(bellybutton),thepainbeginsstomach-high.Astheappendixbecomesmoreswollenandinflamed,itbeginstoirritatetheadjoiningabdominalwall.Thisleadstothelocalizationofthepainto therightlowerquadrant.Thisclassicmigrationofpainmaynotbeseeninchildrenunderthreeyears.Thispaincanbeelicitedthroughvarioussignsandcanbesevere.Signsincludelocalizedfindingsintheright iliacfossa.Theabdominalwallbecomesverysensitivetogentlepressure(palpation).Also,thereisseverepainonsuddenreleaseofdeeppressureinthelowerabdomen(reboundtenderness).Iftheappendixisretrocecal(localizedbehindthe cecum),evendeeppressureintherightlowerquadrantmayfailtoelicittenderness(silentappendix).Thisisbecausethe cecum,distendedwithgas,protectstheinflamedappendixfrompressure.Similarly,iftheappendixliesentirelywithinthepelvis,thereisusuallycompleteabsenceofabdominalrigidity.Insuchcases,adigitalrectalexamination elicitstendernessintherectovesicalpouch.Coughingcausespointtendernessinthisarea(McBurney'spoint).
Causes[edit]
Basedonexperimentalevidence,acuteappendicitisseemstobetheendresultofaprimaryobstructionoftheappendiceal lumen.[18][19] Oncethisobstructionoccurs,theappendixbecomesfilledwith mucus andswells.Thiscontinuedproductionofintra-lumenalmucusleadstoincreasedpressureswithinthelumenandthewallsoftheappendix.Thisincreasedpressureresultsin thrombosis and occlusion ofthesmallvessels,andstasisoflymphaticflow.Atthispointspontaneousrecoveryrarelyoccurs.Astheocclusionofbloodvesselsprogresses,theappendixbecomes ischemic andthen necrotic.As bacteria begintoleakoutthroughthedyingwalls, pus formswithinandaroundtheappendix(suppuration).Theendresultofthiscascadeisappendicealrupture(a'burstappendix')causing peritonitis,whichmayleadto sepsis andeventually death.Thiscascadeofeventsisresponsiblefortheslowlyevolvingabdominalpainandothercommonlyassociatedsymptoms.[9]
Thecausativeagentsinclude bezoars,foreignbodies, trauma, intestinalworms, lymphadenitis,and,mostcommonly,calcifiedfecaldepositsthatareknownasappendicolithsorfecaliths.[20] Theoccurrenceof obstructingfecaliths hasattractedattentionsincetheirpresenceinpersonswithappendicitisishigherindevelopedthanindevelopingcountries.[21] Inadditionanappendicealfecalithiscommonlyassociatedwithcomplicatedappendicitis.[22] Also,fecalstasisandarrestmayplayarole,asdemonstratedbypersonswithacuteappendicitishavingfewerbowelmovementsperweekcomparedwithhealthycontrols.[23][24] Theoccurrenceofafecalithintheappendixwasthoughttobeattributedtoaright-sidedfecalretentionreservoirinthecolonandaprolongedtransittime.Howeveraprolongedtransittimewasnotobservedinsubsequentstudies.[25] Fromepidemiologicaldata,ithasbeenstatedthatdiverticulardiseaseandadenomatouspolypswereunknownandcoloncancerexceedinglyrareincommunitiesexemptfromappendicitis.[26][27] Also,acuteappendicitishasbeenshowntooccurantecedenttocancerinthecolonandrectum.[28]Severalstudiesofferevidencethatalowfiberintakeisinvolvedinthepathogenesisofappendicitis.[29][30][31] Thislowintakeofdietaryfiberisinaccordancewiththeoccurrenceofaright-sidedfecalreservoirandthefactthatdietaryfiberreducestransittime.[32] Perihepatituscanbecausedby pelvicinflammatorydisease.[33]
Diagnosis[edit]
Diagnosisisbasedonamedicalhistory(symptoms)andphysicalexaminationwhichcanbesupportedbyanelevationof neutrophilic whitebloodcellsandimagingstudiesifneeded.(Neutrophilsaretheprimarywhitebloodcellsthatrespondtoabacterialinfection.)Historiesfallintotwocategories,typicalandatypical.Typicalappendicitisincludesseveralhoursofgeneralizedabdominalpainwhichbeginsintheregionoftheumbilicuswithassociated anorexia,nausea,orvomiting.Thepainthen"localizes"intotherightlowerquadrantwherethetendernessincreasesinintensity.Howeveritispossiblethepaincouldlocalizetothe theleftlowerquadrant inpersonswith situsinversustotalis.Thecombinationofpain,anorexia,leukocytosis,andfeverisclassic.Atypicalhistorieslackthistypicalprogressionandmayincludepainintherightlowerquadrantasaninitialsymptom.Irritationoftheperitoneum(insideliningoftheabdominalwall)canleadtoincreasedpainonmovement,orjolting,forexamplegoingoverspeedbumps.[34] Atypicalhistoriesoftenrequireimagingwithultrasoundand/orCTscanning.[35]
Clinical[edit]
∙Aure-Rozanovasign:
Increasedpainonpalpationwithfingerinright Petittriangle (canbeapositiveShchetkin-Bloomberg's)
∙Bartomier-Michelson'ssign:
Increasedpainonpalpationattherightiliacregionasthepersonbeingexaminedliesonhis/herleftsidecomparedtowhenhe/sheliesonhis/herback.
∙Dunphy'ssign:
Increasedpainintherightlowerquadrantwithcoughing.[36]
∙Kocher's(Kosher's)sign:
Fromtheperson'smedicalhistory,thestartofpainintheumbilicalregionwithasubsequentshifttotherightiliacregion.
∙Massouhsign:
DevelopedinandpopularinsouthwestEngland,theexaminerperformsafirmswishwithhis/herindexandmiddlefingeracrosstheabdomenfromthe Xiphoidprocess totheleftandtherightiliacfossa.ApositiveMassouhsignisagrimaceofthepersonbeingexamineduponarightsided(andnotleft)sweep.
∙Obturatorsign:
Thepersonbeingevaluatedliesonher/hisbackwiththehipandkneebothflexedatninetydegrees.Theexaminerholdstheperson'sanklewithonehandandkneewiththeotherhand.Theexaminerrotatesthehipbymovingtheperson'sankleawayfromthehis/herbodywhileallowingthekneetomoveonlyinward.Apositivetestispainwithinternalrotationofthehip.
∙Psoassign:
Alsoknownasthe"Obraztsova'ssign"isrightlower-quadrantpainthatisproducedwitheitherthepassiveextensionoftherighthiporbytheactiveflexionoftheperson'srighthipwhilesupine.Thepainthatiselicitedisdue
 升级会员
升级会员 